Behavioral Insomnia of Childhood

For many families, the struggle to achieve a full night’s rest feels like an inevitable rite of passage. However, when sleep challenges become chronic, they often cross the threshold into a clinical diagnosis known as Behavioral Insomnia of Childhood (BIC).
Recognized by the International Classification of Sleep Disorders (ICSD-3), BIC is not a physiological "malfunction" but rather a set of learned behaviors and environmental conditions that disrupt sleep. It affects approximately 20% to 30% of children and is defined by its extrinsic nature—meaning the problem is usually rooted in how sleep is initiated or maintained rather than a biological disorder.
The Three Clinical Subtypes of BIC
To treat BIC effectively, we must first categorize the behavior. Clinicians generally identify three distinct presentations:
Sleep-Onset Association Type: This is the most common form in infants. The child becomes dependent on a specific object, person, or activity to fall asleep (e.g., being rocked, nursing, or a pacifier). When they naturally wake between sleep cycles—as all humans do—they lack the skills to "self-soothe" and return to sleep without that same external cue.
Limit-Setting Type: Primarily seen in toddlers and preschoolers. This manifests as stalling tactics or "curtain calls" (requests for another glass of water, one more hug). It occurs when a caregiver is unable or unwilling to enforce consistent bedtime boundaries.
Combined Type: As the name suggests, this is a blend of both. A child may require a parent’s presence to fall asleep (association) while simultaneously engaging in stalling behaviors to delay the process (limit-setting).
Developmental Perspectives: Infants vs. Toddlers
The experience—and the solution—shifts as the child grows.
Infants (after 2 months): The perspective here is biological and regulatory. Infants forms neurological associations. If they always fall asleep while feeding, their brain literally codes "feeding" as a prerequisite for sleep. The goal at this age is to shift from external regulation to internal self-soothing.
Note: in the first few months of life (typically 0–3 months), infants follow an ultradian rhythm—short bursts of sleep and wakefulness driven primarily by hunger and homeostatic sleep pressure. You can’t technically have "insomnia" in a newborn because their sleep isn't organized enough to be "disrupted" in a behavioral sense; it’s just biologically fragmented.
Toddlers & Young Children: The perspective shifts toward autonomy and social interaction. Toddlers are developmentally programmed to seek independence and test the limits of their environment. Sleep is often viewed as a separation from the family or a "fear of missing out," leading to more complex behavioral resistance. Learn more about separation anxiety and co-regulation: here.
As of today (year 2026), the consensus remains that behavioral interventions are the first-line treatment, boasting a success rate of approximately 94% in clinical reviews.
Digital & Remote Interventions (The "Digital Shift")
Current research has pivoted toward accessibility. Digital and Remote Interventions (mHealth) have been validated as highly effective. Telehealth modules and wearable-integrated apps now allow parents to receive professional guidance without visiting a sleep clinic. These tools provide objective data, helping parents see progress that they might miss due to the fog of sleep deprivation.
Global Promise: A 2026 scoping review (University of Miami) found that digital tools—including apps, web modules, and wearable-integrated dashboards—consistently improve total sleep duration and reduce night wakings.
Peer Support Synergy: Research indicates that online programs are significantly more effective when paired with digital peer support groups (e.g., moderated social media communities), which improve parental adherence.
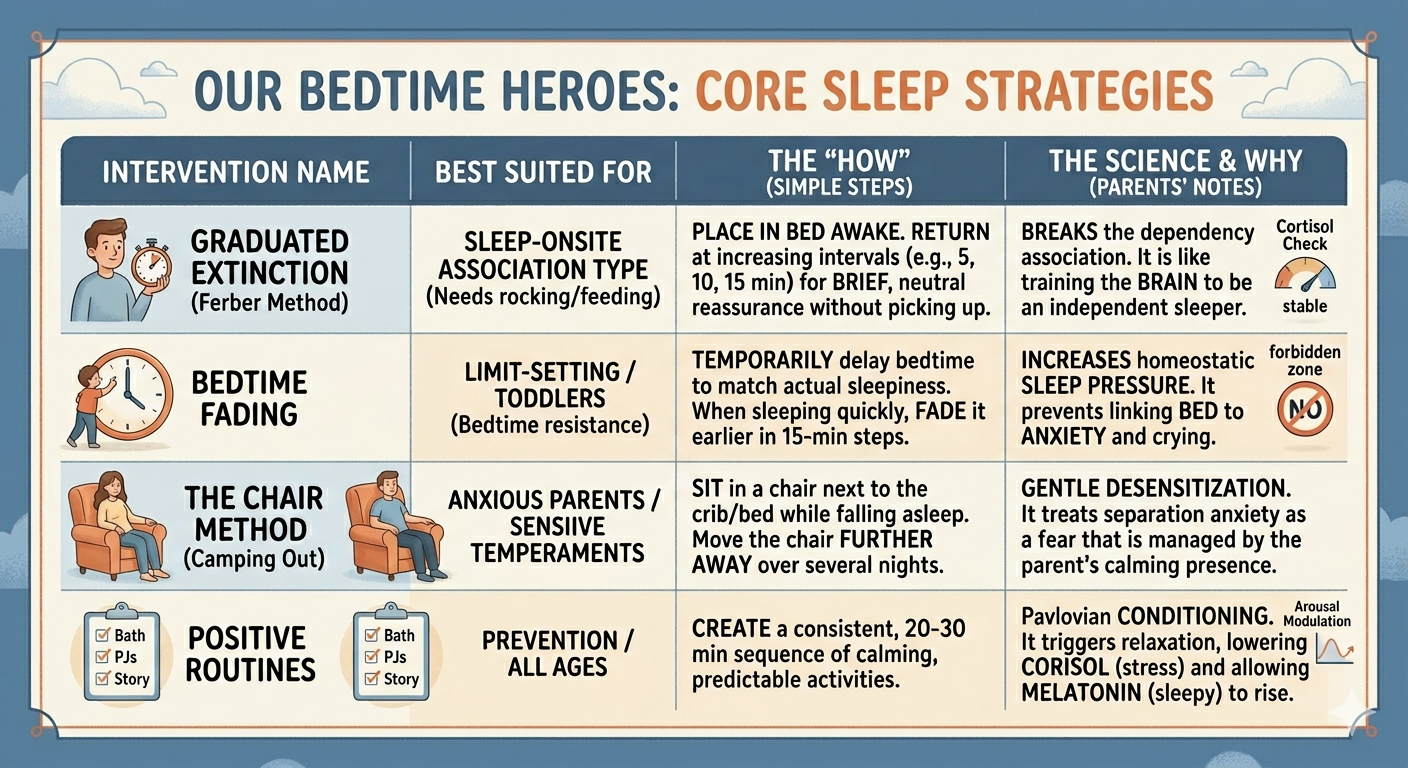
Core Evidence-Based Interventions
Below is a breakdown of how these interventions map to the clinical subtypes:
Graduated Extinction: Checking on the child at increasing intervals (e.g., the Ferber method).
Best Suited For: Sleep-Onset Association
How:
Place the child in bed at their usual time. If they cry, you return at predetermined, increasing intervals (e.g., 5 minutes, 10 minutes, 15 minutes) to provide brief, neutral reassurance without picking them up.
Science and Why:
In many BIC cases, parental presence (rocking, patting, or nursing) acts as a Positive Reinforcer for crying. In other words, the crying protest behavior is rewarded by parental presence/return. By gradually withdrawing the reward (reinforcer), the behavior eventually disappears (extinguishes).
Unlike unmodified extinction, the "graduated" check-ins are designed to reduce parental stress and provide periodic reassurance to the child, while still preventing the reinforcement of the sleep-onset association.
Bedtime Fading: Delaying bedtime to match kid’s natural sleepiness, then moving it earlier.
Best Suited For: Limit-Setting / Toddlers
How:
You temporarily move the child's bedtime much later—to the time they actually fall asleep naturally (e.g., moving an 8:00 PM bedtime to 9 or even 9:30 PM). Because they are exhausted, they fall asleep almost instantly. Once they associate the bed with fast sleep, you slowly "fade" the bedtime earlier in 15-minute increments.
Science and Why:
This approach starts by temporarily delaying bedtime to match the child's natural sleep onset and then "fading" it earlier in increments. By temporarily delaying bedtime to match when the child is biologically ready for sleep, we maximize their homeostatic sleep pressure (the biological drive for sleep). This ensures they transition to sleep quickly, drastically decreasing protest time in bed.
The main goal is to prevent the kid from linking bed to anxiety and crying. If a child spends two hours crying in bed, the bed becomes a linked stimulus for crying. Bedtime fading uses the high sleep pressure to ensure the bed only triggers the response of sleep, effectively "resetting" the child's psychological relationship with their crib or bed.
Chair Method: Gradually moving the parent's chair further from the crib/bed.
Best Suited For: Anxious Parents / Transitioning
How:
The parent sits in a chair next to the crib/bed while the child falls asleep, gradually moving the chair further away over several nights until they are out of the room. More detailed how has been introduced: here.
Science and Why:
This is based on Gradual Desensitization. It treats the "separation anxiety" or "fear of the dark" as a phobia that is mitigated by the parent’s presence. By slowly withdrawing the "safety cue" (the parent), the child learns to tolerate the sleep environment independently.
No matter which sleep-training method you are using, never forget the importance in sleep ritual/routine.
The Parent's Mind: The Implementation Barrier
One of the most critical findings in recent sleep research is that the success of these methods depends largely on parental cognition. The PUMBA-Q Scale has helped clinicians identify that parental anxiety—specifically the fear that "crying" causes harm—is the primary reason interventions fail.
When parents understand the Safety and Neurodevelopmental Outcomes, they are more likely to stay consistent:
No Long-Term Harm: Decades of follow-up studies confirm that behavioral interventions do not damage parent-child attachment or psychological health.
The Stress Paradox: Research using salivary cortisol markers shows that chronically sleep-deprived infants actually have higher stress levels than those who have undergone sleep training. Consolidated sleep helps regulate the HPA axis (the body's stress response system), making the child more resilient in the long run.
Ultimately, these findings suggest that the most significant barrier to a child’s sleep is often not the child’s behavior, but the parent’s emotional resolve. By reframing "crying" from a sign of harm to a temporary byproduct of a health-promoting process, parents can shift their perspective from guilt to empowerment.
Conclusion
Treating Behavioral Insomnia of Childhood is not about "forcing" a child to sleep, but about creating the environmental and behavioral scaffolding they need to overcome Behavioral Insomnia of Childhood. By recognizing the specific subtype and utilizing modern digital tools and evidence-based routines, parents can foster a healthier sleep environment for the entire family.
-
Mindell, J. A., Kuhn, B., Lewin, D. S., Meltzer, L. J., & Sadeh, A. (2006). Behavioral treatment of bedtime problems and night wakings in infants and young children. Sleep, 29(10), 1263–1276.
Morgenthaler, T. I., et al. (2006). Practice Parameters for the Behavioral Treatment of Bedtime Problems and Night Wakings in Infants and Young Children. Sleep, 29(10), 1277–1281.
Meltzer, L. J., & Mindell, J. A. (2014). Systematic review and meta-analysis of behavioral interventions for pediatric insomnia. Journal of Pediatric Psychology, 39(8), 932–948.
Gradisar, M., et al. (2016). Behavioral Interventions for Infant Sleep: A Randomized Controlled Trial. Pediatrics, 137(6).
Piazza, C. C., & Fisher, W. (1991). A faded bedtime with response cost protocol for treatment of multiple sleep problems in children. Journal of Applied Behavior Analysis, 24(1), 129–140.
Ashbaugh, R., & Peck, S. M. (1998). Treatment of sleep problems in a toddler: A replication of the faded bedtime with response cost protocol. Journal of Applied Behavior Analysis, 31(1), 127–129.
LeBourgeois, M. K., et al. (2013). Circadian Phase and Its Relationship to Nighttime Sleep in Toddlers. Sleep Medicine, 14(8), 712–720.
Mindell, J. A., et al. (2009). A Nightly Bedtime Routine: Impact on Sleep in Young Children and Maternal Mood. Sleep, 32(5), 599–606.